Monday, 15 March 2021
Wednesday, 19 August 2020
PDX
Selection of Principal Diagnosis
The circumstances of inpatient admission always govern the selection of principal diagnosis. The principal diagnosis is defined in the Uniform Hospital Discharge Data Set (UHDDS) as “that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care.”
The UHDDS definitions are used by hospitals to report inpatient data elements in a standardized manner. These data elements and their definitions can be found in the July 31, 1985, Federal Register (Vol. 50, No, 147), pp. 31038-40.
Since that time the application of the UHDDS definitions has been expanded to include all non-outpatient settings (acute care, short term, long term care and psychiatric hospitals; home health agencies; rehab facilities; nursing homes, etc). The UHDDS definitions also apply to hospice services (all levels of care).
In determining principal diagnosis, coding conventions in the ICD-10-CM, the Tabular List and Alphabetic Index take precedence over these official coding guidelines.
The importance of consistent, complete documentation in the medical record cannot be overemphasized. Without such documentation the application of all coding guidelines is a difficult, if not impossible, task.
A. Codes for symptoms, signs, and ill-defined conditions
Codes for symptoms, signs, and ill-defined conditions from Chapter 18 are not to be used as principal diagnosis when a related definitive diagnosis has been established.
B. Two or more interrelated conditions, each potentially meeting the definition for principal diagnosis.
When there are two or more interrelated conditions (such as diseases in the same ICD-10-CM chapter or manifestations characteristically associated with a certain disease) potentially meeting the definition of principal diagnosis, either condition may be sequenced first, unless the circumstances of the admission,
the therapy provided, the Tabular List, or the Alphabetic Index indicate otherwise.
C. Two or more diagnoses that equally meet the definition for principal diagnosis
In the unusual instance when two or more diagnoses equally meet the criteria for principal diagnosis as determined by the circumstances of admission, diagnostic workup and/or therapy provided, and the Alphabetic Index, Tabular List, or another coding guidelines does not provide sequencing direction, any one of the diagnoses may be sequenced first.
D. Two or more comparative or contrasting conditions
In those rare instances when two or more contrasting or comparative diagnoses are documented as “either/or” (or similar terminology), they are coded as if the diagnoses were confirmed and the diagnoses are sequenced according to the circumstances of the admission. If no further determination can be made as to which diagnosis should be principal, either diagnosis may be sequenced first.
F. Original treatment plan not carried out
Sequence as the principal diagnosis the condition, which after study occasioned the admission to the hospital, even though treatment may not have been carried out due to unforeseen circumstances.
G. Complications of surgery and other medical care
When the admission is for treatment of a complication resulting from surgery or other medical care, the complication code is sequenced as the principal diagnosis. If the complication is classified to the T80-T88 series and the code lacks the necessary specificity in describing the complication, an additional code for the specific complication should be assigned.
H. Uncertain Diagnosis
If the diagnosis documented at the time of discharge is qualified as “probable,” “suspected,” “likely,” “questionable,” “possible,” or “still to be ruled out,” “compatible with,” “consistent with,” or other similar terms indicating uncertainty, code the condition as if it existed or was established. The bases for these guidelines are the diagnostic workup, arrangements for further workup or
observation, and initial therapeutic approach that correspond most closely with the established diagnosis.
Note: This guideline is applicable only to inpatient admissions to short-term, acute, long-term care and psychiatric hospitals.
I. Admission from Observation Unit
1. Admission Following Medical Observation
When a patient is admitted to an observation unit for a medical condition, which either worsens or does not improve, and is subsequently admitted as an inpatient of the same hospital for this same medical condition, the principal diagnosis would be the medical condition which led to the hospital admission.
2. Admission Following Post-Operative Observation
When a patient is admitted to an observation unit to monitor a condition (or complication) that develops following outpatient surgery, and then is subsequently admitted as an inpatient of the same hospital, hospitals should apply the Uniform Hospital Discharge Data Set (UHDDS) definition of principal diagnosis as "that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care."
J. Admission from Outpatient Surgery
When a patient receives surgery in the hospital's outpatient surgery department and is subsequently admitted for continuing inpatient care at the same hospital, the following guidelines should be followed in selecting the principal diagnosis for the inpatient admission:
• If the reason for the inpatient admission is a complication, assign the complication as the principal diagnosis.
• If no complication, or other condition, is documented as the reason for the inpatient admission, assign the reason for the outpatient surgery as the principal diagnosis.
• If the reason for the inpatient admission is another condition unrelated to the surgery, assign the unrelated condition as the principal diagnosis.
Section III. Reporting Additional Diagnoses
GENERAL RULES FOR OTHER (ADDITIONAL) DIAGNOSES
For reporting purposes the definition for “other diagnoses” is interpreted as additional conditions that affect patient care in terms of requiring:
clinical evaluation; or
therapeutic treatment; or
diagnostic procedures; or
extended length of hospital stay; or
increased nursing care and/or monitoring.
The UHDDS item #11-b defines Other Diagnoses as “all conditions that coexist at the time of admission, that develop subsequently, or that affect the treatment received and/or the length of stay. Diagnoses that relate to an earlier episode which have no bearing on the current hospital stay are to be excluded.” UHDDS definitions apply to inpatients in acute care, short-term, long term care and psychiatric hospital setting. The UHDDS definitions are used by acute care short-term hospitals to report inpatient data elements in a standardized manner. These data elements and their definitions can be found in the July 31, 1985, Federal Register (Vol. 50, No, 147), pp. 31038-40.
Since that time the application of the UHDDS definitions has been expanded to include all non-outpatient settings (acute care, short term, long term care and psychiatric hospitals; home health agencies; rehab facilities; nursing homes, etc). The UHDDS definitions also apply to hospice services (all levels of care).
The following guidelines are to be applied in designating “other diagnoses” when neither the Alphabetic Index nor the Tabular List in ICD-10-CM provide direction. The listing of the diagnoses in the patient record is the responsibility of the attending provider.
A. Previous conditions
If the provider has included a diagnosis in the final diagnostic statement, such as the discharge summary or the face sheet, it should ordinarily be coded. Some providers include in the diagnostic statement resolved conditions or diagnoses and status-post procedures from previous admission that have no bearing on the current stay. Such conditions are not to be reported and are coded only if required by hospital policy.
However, history codes (categories Z80-Z87) may be used as secondary codes if the historical condition or family history has an impact on current care or influences treatment.
B. Abnormal findings
Abnormal findings (laboratory, x-ray, pathologic, and other diagnostic results) are not coded and reported unless the provider indicates their clinical significance. If the findings are outside the normal range and the attending provider has ordered other tests to evaluate the condition or prescribed
treatment, it is appropriate to ask the provider whether the abnormal finding should be added.
Please note: This differs from the coding practices in the outpatient setting for coding encounters for diagnostic tests that have been interpreted by a provider.
C. Uncertain Diagnosis
If the diagnosis documented at the time of discharge is qualified as “probable,” “suspected,” “likely,” “questionable,” “possible,” or “still to be ruled out,” “compatible with,” “consistent with,” or other similar terms indicating uncertainty, code the condition as if it existed or was established. The bases for these guidelines are the diagnostic workup, arrangements for further workup or observation, and initial therapeutic approach that correspond most closely with the established diagnosis.
Note: This guideline is applicable only to inpatient admissions to short-term, acute, long-term care and psychiatric hospitals.
Tuesday, 18 August 2020
Coding Clinic
Coding Clinic for ICD-10-CM and ICD-10-PCS is the quarterly newsletter published by the American Hospital Association's Central Office on ICD-10-CM and ICD-10-PCS. The advice provided in Coding Clinic is the result of a formal cooperative effort between the American Hospital Association (AHA), the American Health Information Management Association (AHIMA), the Centers for Disease Control and Prevention (CDC) National Center for Health Statistics (NCHS) and the Centers for Medicare and Medicaid Services (CMS). In addition to these organizations, the Editorial Advisory Board consists of an expert panel of physicians representing the American Medical Association, the American College of Surgeons, the American Academy of Pediatrics and the American College of Physicians, as well as coding professionals representing healthcare facilities.
AHA Coding Clinic for ICD is the official source for ICD (ICD-10-CM/PCS) coding advice to supplement and clarify the Official Guidelines for Coding and Reporting.
Coding Clinic is published quarterly by the American Hospital Association (AHA) Central Office.
Official coding advice and official coding guidelines.
Correct code assignments for new technologies and newly identified diseases.
Articles and topics which will offer practical information and improve data quality.
Provides
information about coding changes and/or corrections to hospitals and other
parties.
Tuesday, 11 August 2020
Query Process
A query is a communication between the provider (Physician) and Medical Coder to clarify documentation in the health record for documentation integrity and accurate code assignment for an individual encounter in any healthcare setting.
A query will include information like; Patient name, Admission date and/or date of service, Medical record number, Date query initiated, Date query answered, Name and contact information of the individual initiating the query
A query should have statement of the issue in the form of a question along with clinical indicators specified from the patient’s record.
Types of Query:
POA query, Ruled in /ruled out query, Clinical significance query, Cause and effect query, Conflicting documentation query, CHF acuity and specificity query, Debridement type and depth query.
Sunday, 9 August 2020
Starting career as Medical Coder
Medical coding is the process of converting medical diagnosis, symptoms, procedures, and/or drugs into codes. Medical coders ensure that medical information is transmitted accurately and efficiently between healthcare providers and insurance payers. Physicians and hospitals depend on accurate coding to receive proper reimbursement, making the role of the coder a valued one.
Medical coders work in all types of healthcare facilities, including doctor’s offices, clinics, hospitals and health care systems.
Thus Medical Coders play pivotal role in the financial success of Healthcare Centers. The greater the expertise of the Medical Coder in identifying relevant diagnoses for patient encounters, the greater the insurance reimbursement to the physician.
There is massive demand for medical coders throughout the World. The number of people covered under medical insurance is growing rapidly, so there is growing demand from hospitals for coders who can electronically maintain patients’ records and liaise with medical insurance companies for claims processing.
Eligibility: Graduates from sectors like science, B.Pharmacy, M.Pharmacy, nursing, biotechnology, microbiology or physiotherapy are eligible to pursue diploma/certificate programmes in medical coding offered by institutions accredited by the US-based American Health Information Management Association (AHIMA) and American Academy of Professional Coders (AAPC).
Certified Medical Coders are in high currently.
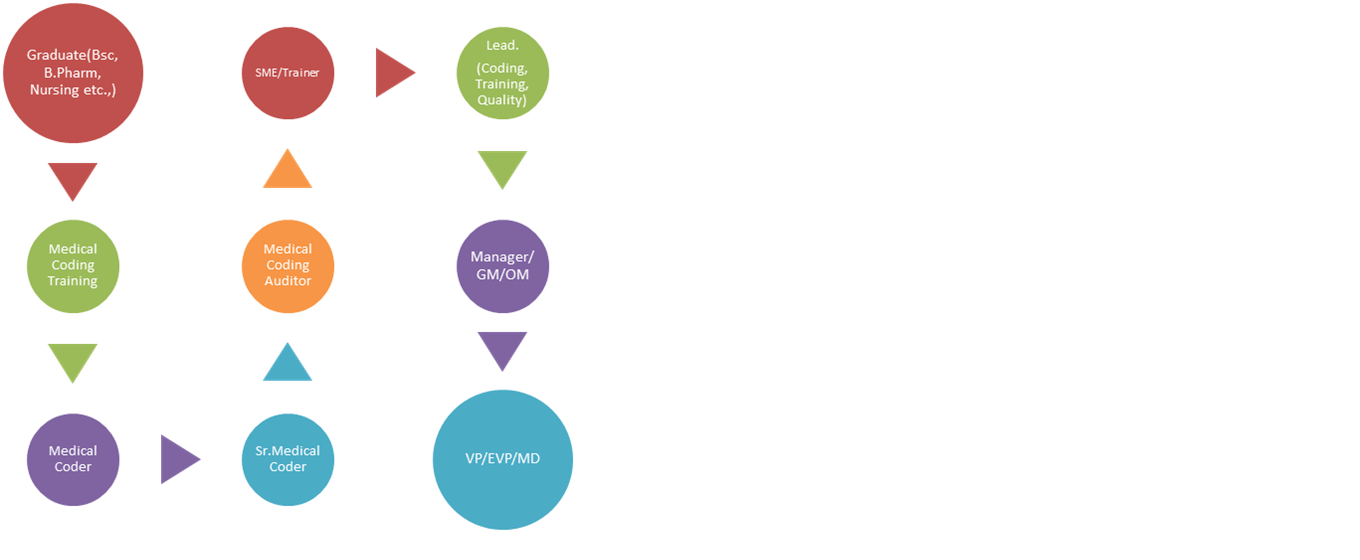
Pay-scale: Fresh graduates from the above said streams can expect an average salary of INR 12,000 to INR 20,000 per month. After 5 to 6 years of experience, a medical coder can expect a salary of INR 35,000 to 50,000 and growth in position to a Lead and then Manager, Sr.Manager followed by GM etcetera.
What Is the Future Outlook for the Medical Coding Industry?
Medical coding and billing careers offer health information technicians favorable job prospects, to say the least. The demand is so high that the U.S. Bureau of Labor Statistics lists medical coding among the 20 fastest growing occupations.
The Affordable Care Act has played a role in the demand for medical coders by ensuring that more people are eligible for medical care. In 2018, according to the most recent stats from the Centers for Disease Control and Prevention (CDC), “more” is defined as upwards of 1.4 billion patient visits in that year. Considering every patient encounter by every healthcare provider requires coded documentation and records, it’s not surprising that medical coding is among the most sought-after healthcare careers.
Job security factors into quality of life, which is one reason why medical coding is a good career choice. Despite economic fluctuations impacting employment opportunities for most professions, the need for healthcare professionals, including health information technicians, is at a historic high—and will remain so.
(Source: https://www.aapc.com/resources/research/medical-coding-salary-survey/)
Sunday, 26 July 2020
COVID-19 Coding
Code only a confirmed diagnosis of COVID-19 as documented by the provider, documentation of a positive COVID-19 test result.
A presumptive positive COVID-19 test result should be coded as confirmed COVID-19 infection.
For a confirmed diagnosis, assign code U07.1, COVID-19
Confirmation does not require documentation of the type of test performed; the provider’s documentation that the individual has COVID-19 is sufficient.
Sequencing of codes:
When COVID-19 meets the definition of principal diagnosis, code U07.1, COVID-19, should be sequenced first, followed by the appropriate codes for associated manifestations, except in the case of obstetrics patients as indicated in Section . I.C.15.s. for COVID-19 in pregnancy, childbirth, and the puerperium.
Acute respiratory illness due to COVID-19 :
(i) Pneumonia:
For a pneumonia case confirmed as due to the 2019 novel coronavirus (COVID-19), assign codes U07.1, COVID-19, and J12.89, Other viral pneumonia.
(ii) Acute bronchitis:
For a patient with acute bronchitis confirmed as due to COVID-19, assign codes U07.1, and J20.8, Acute bronchitis due to other specified organisms. Bronchitis not otherwise specified (NOS) due to COVID-19 should be coded using code U07.1 and J40, Bronchitis, not specified as acute or chronic.
(iii) Lower respiratory infection:
If the COVID-19 is documented as being associated with a lower respiratory infection, not otherwise specified (NOS), or an acute respiratory infection, NOS, codes U07.1 and J22, Unspecified acute lower respiratory infection, should be assigned.
If the COVID-19 is documented as being associated with a respiratory infection, NOS, codes U07.1 and J98.8, Other specified respiratory disorders, should be assigned.
(iv) Acute respiratory distress syndrome:
For acute respiratory distress syndrome (ARDS) due to COVID-19, assign codes U07.1, and J80, Acute respiratory distress syndrome.
Exposure to COVID-19:
For cases where there is a concern about a possible exposure to COVID-19, but this is ruled out after evaluation, assign code Z03.818, Encounter for observation for suspected exposure to other biological agents ruled out.
For cases where there is an actual exposure to someone who is confirmed or suspected (not ruled out) to have COVID-19, and the exposed individual either tests negative or the test results are unknown, assign code Z20.828, Contact with and (suspected) exposure to other viral communicable diseases.
Screening for COVID-19:
For asymptomatic individuals who are being screened for COVID-19 and have no known exposure to the virus, and the test results are either unknown or negative, assign code Z11.59, Encounter for screening for other viral diseases. For individuals who are being screened due to a possible or actual exposure to COVID-19.
Asymptomatic individuals tested positive for COVID-19:
For asymptomatic individuals who test positive for COVID-19, assign code U07.1, COVID-19.
Pregnancy, Childbirth, and the Puerperium:
COVID-19 infection in pregnancy, childbirth, and the puerperium During pregnancy, childbirth or the puerperium, a patient admitted because of COVID-19 should receive a principal diagnosis code of O98.5-, Other viral diseases complicating pregnancy, childbirth and the puerperium, followed by code U07.1, COVID-19, and the appropriate codes for associated manifestation(s).
HAPPY CODING.......................,,,
Sunday, 17 May 2020
CHF (Congestive Heart Failure)
Medications:

Saturday, 16 May 2020
Common Medical Specialists
A SPECIALTY is a branch of medicine that is focused on a defined group of diseases, patients, or skills.
Anesthesiologist:
Friday, 15 May 2020
Frequently Used Medical Terms in In-patient DRG coding
Wednesday, 13 May 2020
Sepsis
Wednesday, 29 April 2020
Present On Admission or POA
POA stands for Present On Admission, meaning, whether a condition was present at the time of In-patient admission or not.
CMS defines POA as PRESENT AT THE TIME THE ORDER FOR INPATIENT ADMISSION OCCURS.
POA Indicators
Y = Yes (Present at the time of inpatient admission)
N = No (Not present at the time of inpatient admission)
U = Unknown (Documentation is insufficient to determine if the condition was present at the time of inpatient admission)
W = Clinically undetermined (Provider is unable to clinically determine whether the condition was present at the time of inpatient admission or not)
Issues related to inconsistent, missing, conflicting, or unclear documentation are resolved by the provider as a result of the physical query process.
Sunday, 3 November 2019
What is Medical Coding...
Medical Coding is the process of converting healthcare diagnoses, procedures, medical supplies/services, and equipment into alphanumeric codes. The diagnoses,procedures and services provided are abstracted from medical records that may either be paper or EHR (Electronic Health Record).

ICD (International Classification of Diseases) guidelines (set of rules to follow while assigning codes) are used to abstract the diagnoses from the medical records. These guidelines are developed by CMS (Centers for Medicare and Medicaid
Services and NCHS (National Center for Health Statistics, who are part of the U.S. Federal Government’s Department of Health and Human Services.
ICD guidelines have been approved by the four organizations that make up the Cooperating Parties: The American Hospital Association, American Health Information Management Association, CMS, and NCHS.
The ICD guideline are revised annually and the updated guidelines will be published and will become effective from 1st October of every year.
More than 100 countries are using ICD guidelines to process the medical codes. Few countries have modified the guidelines according to their local Healthcare System requirements. ICD 10-CM is used by The USA, Canada and few Middle East countries whereas ICD 10-AM is used in Australia, New Zealand, Singapore, Saudi Arabia, Qatar, Kuwait etc. UK has got their own modification of ICD guidelines.
Wednesday, 23 October 2019
Medical Terms
Medical terminology contain 3 main parts. If you are aware of these 3 it will be easy for you to understand simple to complex medical/clinical terms.
Root word GASTR | ITIS suffix
Related to inflammation
stomach
Prefix: The term before the root word.
Root word: The main term you are pointing to/related to organs/systems/parts/procedures.
Suffix: The term at the end of root word.
ab- away from (abduction)
abdomin/o abdomen
A few of the frequently used medical terms in In-patient DRG coding......
-
 The Diagnosis Related Group (DRG): A patient classification system, which provides a means of relating the type of patients a hospital tr...
The Diagnosis Related Group (DRG): A patient classification system, which provides a means of relating the type of patients a hospital tr... -
COVID-19 Infections (Infections due to SARS-CoV-2) Code only a confirmed diagnosis of COVID-19 as documented by the provider, documentati...
-
A SPECIALTY is a branch of medicine that is focused on a defined group of diseases, patients, or skills. Anesthesiologist: Doctor...