Medical coding is the process of converting medical diagnosis, symptoms, procedures, and/or drugs into codes. Medical coders ensure that medical information is transmitted accurately and efficiently between healthcare providers and insurance payers. Physicians and hospitals depend on accurate coding to receive proper reimbursement, making the role of the coder a valued one.
Medical coders work in all types of healthcare facilities, including doctor’s offices, clinics, hospitals and health care systems.
Thus Medical Coders play pivotal role in the financial success of Healthcare Centers. The greater the expertise of the Medical Coder in identifying relevant diagnoses for patient encounters, the greater the insurance reimbursement to the physician.
There is massive demand for medical coders throughout the World. The number of people covered under medical insurance is growing rapidly, so there is growing demand from hospitals for coders who can electronically maintain patients’ records and liaise with medical insurance companies for claims processing.
Eligibility: Graduates from sectors like science, B.Pharmacy, M.Pharmacy, nursing, biotechnology, microbiology or physiotherapy are eligible to pursue diploma/certificate programmes in medical coding offered by institutions accredited by the US-based American Health Information Management Association (AHIMA) and American Academy of Professional Coders (AAPC).
Certified Medical Coders are in high currently.
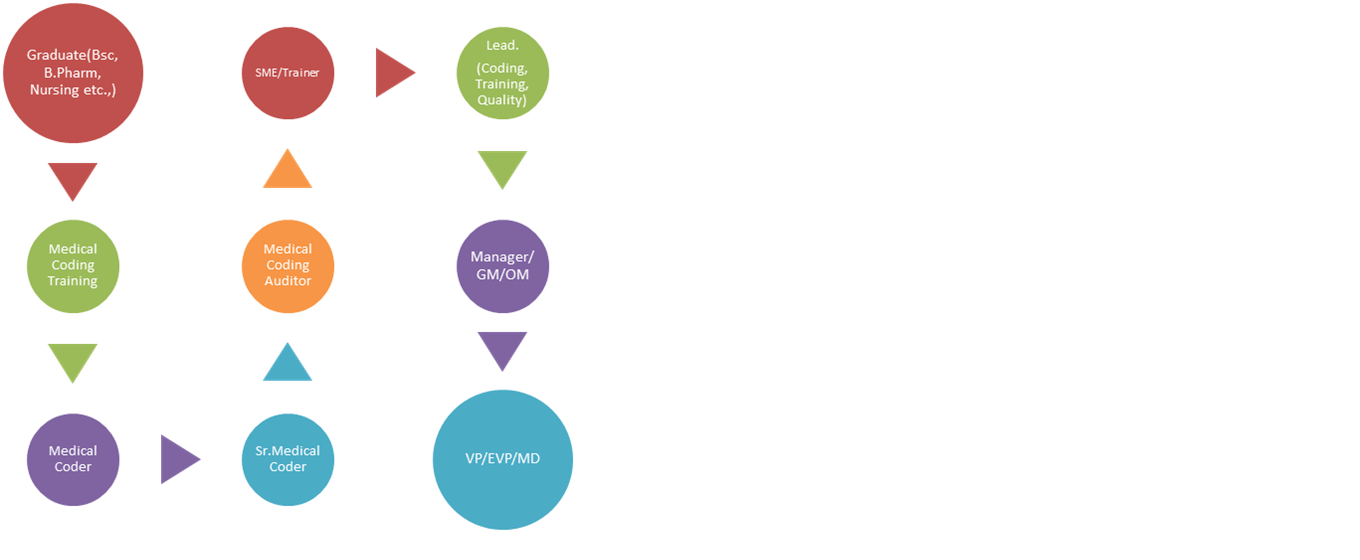
Pay-scale: Fresh graduates from the above said streams can expect an average salary of INR 12,000 to INR 20,000 per month. After 5 to 6 years of experience, a medical coder can expect a salary of INR 35,000 to 50,000 and growth in position to a Lead and then Manager, Sr.Manager followed by GM etcetera.
What Is the Future Outlook for the Medical Coding Industry?
Medical coding and billing careers offer health information technicians favorable job prospects, to say the least. The demand is so high that the U.S. Bureau of Labor Statistics lists medical coding among the 20 fastest growing occupations.
The Affordable Care Act has played a role in the demand for medical coders by ensuring that more people are eligible for medical care. In 2018, according to the most recent stats from the Centers for Disease Control and Prevention (CDC), “more” is defined as upwards of 1.4 billion patient visits in that year. Considering every patient encounter by every healthcare provider requires coded documentation and records, it’s not surprising that medical coding is among the most sought-after healthcare careers.
Job security factors into quality of life, which is one reason why medical coding is a good career choice. Despite economic fluctuations impacting employment opportunities for most professions, the need for healthcare professionals, including health information technicians, is at a historic high—and will remain so.
(Source: https://www.aapc.com/resources/research/medical-coding-salary-survey/)